COVID-19
(Coronavirus disease 2019)
Abstract: COVID-19, also known as Coronavirus disease, is a respiratory infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV 2). Transmission mainly occurs via direct contact or aerosol droplets. The infection may present asymptomatically or with fever and dry cough. Individuals who are over 65 years of age, immunosuppressed, or have preexisting conditions have a higher risk of developing severe symptoms and complications. Management is based on supportive care.
Updated April 7, 2020
Image: by CDC/ Dr. Fred Murphy, License: Public Domain Files
Table of Contents
Etiology
Coronaviruses (CoV) are a family of enveloped, positive-sense, single-stranded RNA (+ssRNA) viruses. They tend to cause mild upper respiratory diseases in humans. Of the 7 known species of CoV, only 3 are known to cause severe infections in humans:
- Severe acute respiratory disease coronavirus (SARS-CoV): emerged in 2003 in southern China from civet cats
- Middle East respiratory syndrome coronavirus (MERS-CoV): emerged in 2012 in Saudi Arabia from dromedary camels
- SARS-CoV 2: emerged in December 2019 in China possibly from bats or pangolins (still under investigation)
Selected diseases caused by Coronaviruses
| Common cold | GI tract infection | Severe acute respiratory syndrome (SARS) | COVID-19 (Wuhan City, China) | |
|---|---|---|---|---|
| Incubation | 3 days | 3 days | 4–6 days | 2–14 days |
| Incidence | Most common | Rare | Rare | ~ 1,200,000 cases (Dec 2019 – April 2020) |
| Prognosis | Complete resolution | Complete resolution (up to 25% fatal for NEC) |
30% resolution 70% severe infection 10% fatal |
80% resolution 15% severe infection 5% critical infection 5.6% fatal (based on confirmed cases as of April 7, 2020, may change) |
| Clinical manifestation | Sneezing, rhinorrhea, headache, sore throat, malaise, fever, chills | Diarrhea, gastroenteritis, neonatal necrotizing enterocolitis |
Fever > 37,8°C (100,0°F), muscle pain, lethargy, cough, sore throat, malaise Shortness of breath/ pneumonia (direct viral or secondary bacterial) |
Asymptomatic Mild infection: fever, dry cough, malaise, dehydration Severe infection: high fever, shortness of breath, chest pain, hemoptysis Complications: pneumonia, ARDS, sepsis, multi-organ failure |
NEC: Necrotizing enterocolitis ARDS: Acute respiratory distress syndrome
The SARS-CoV 2 virion is ~1,250 nm in diameter, and its genome ranges from 26 to 32 kilobases, the largest for an RNA virus. It has 4 structural proteins: spike (S), envelope (E), membrane (M), and nucleocapsid (N).
- N protein forms a complex with RNA and aids in the viral assembly after its replication.
- S, E, and M proteins create the viral envelope.
- S protein, is a club-shaped surface projection, giving the virus its characteristic crown-like appearance on electron microscopy. It’s responsible for viral entry into the human cell.
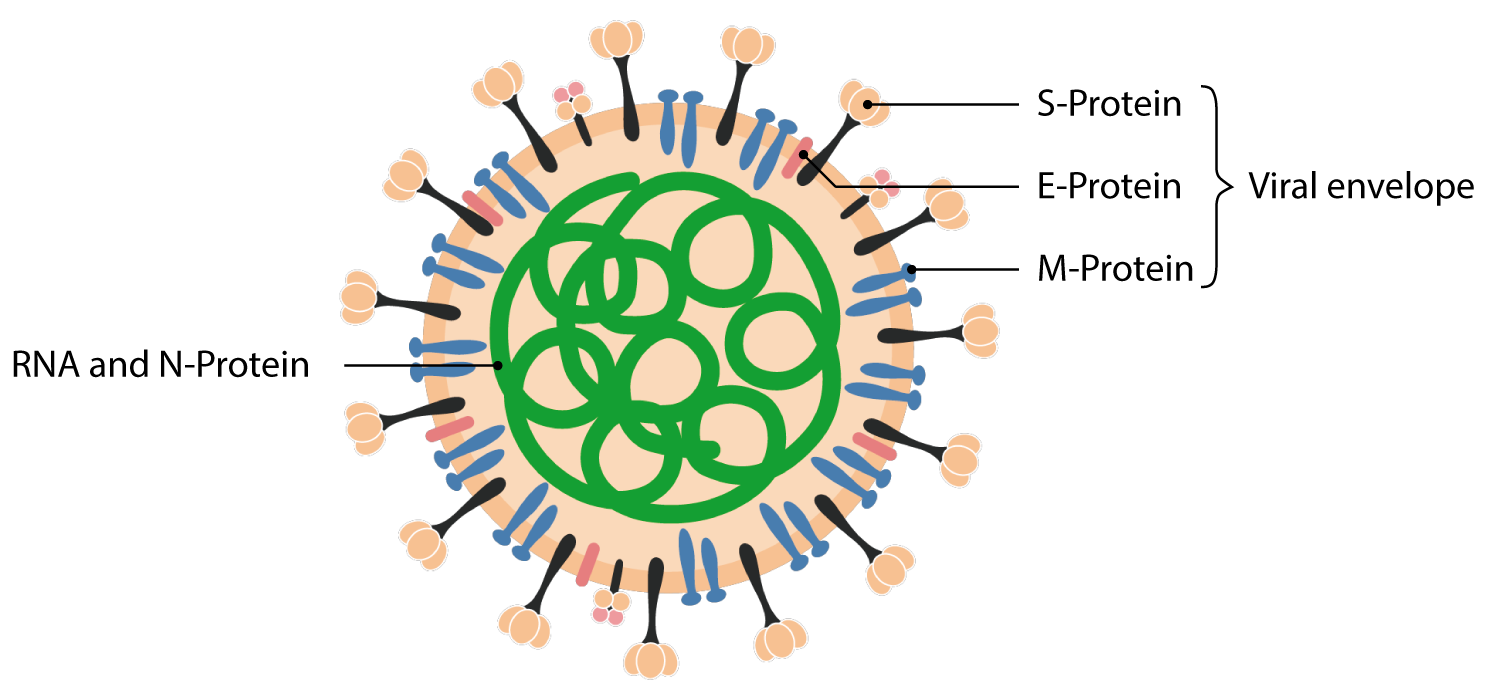
Image: by Lecturio
SARS-CoV 2 attaches to the host cell by binding its S proteins to the receptor protein, angiotensin-converting enzyme 2 (ACE2). ACE2 is expressed by epithelial cells of the intestine, kidney, blood vessels, and most abundantly in type II alveolar cells of the lungs. The virus induces a drop of ACE2 in human cells, possibly inducing lung damage.
The human enzyme transmembrane protease, serine 2 (TMPRSS2) is also used by the virus for S protein priming and to aid in membrane fusion.
Related Video Courses:


Transmission
CoV are zoonotic or transmitted to humans through animals. It is hypothesized that horseshoe bats are the natural reservoir of SARS-CoV 2 since its genome is 97% identical to that of a bat coronavirus. The intermediate host is still unknown.
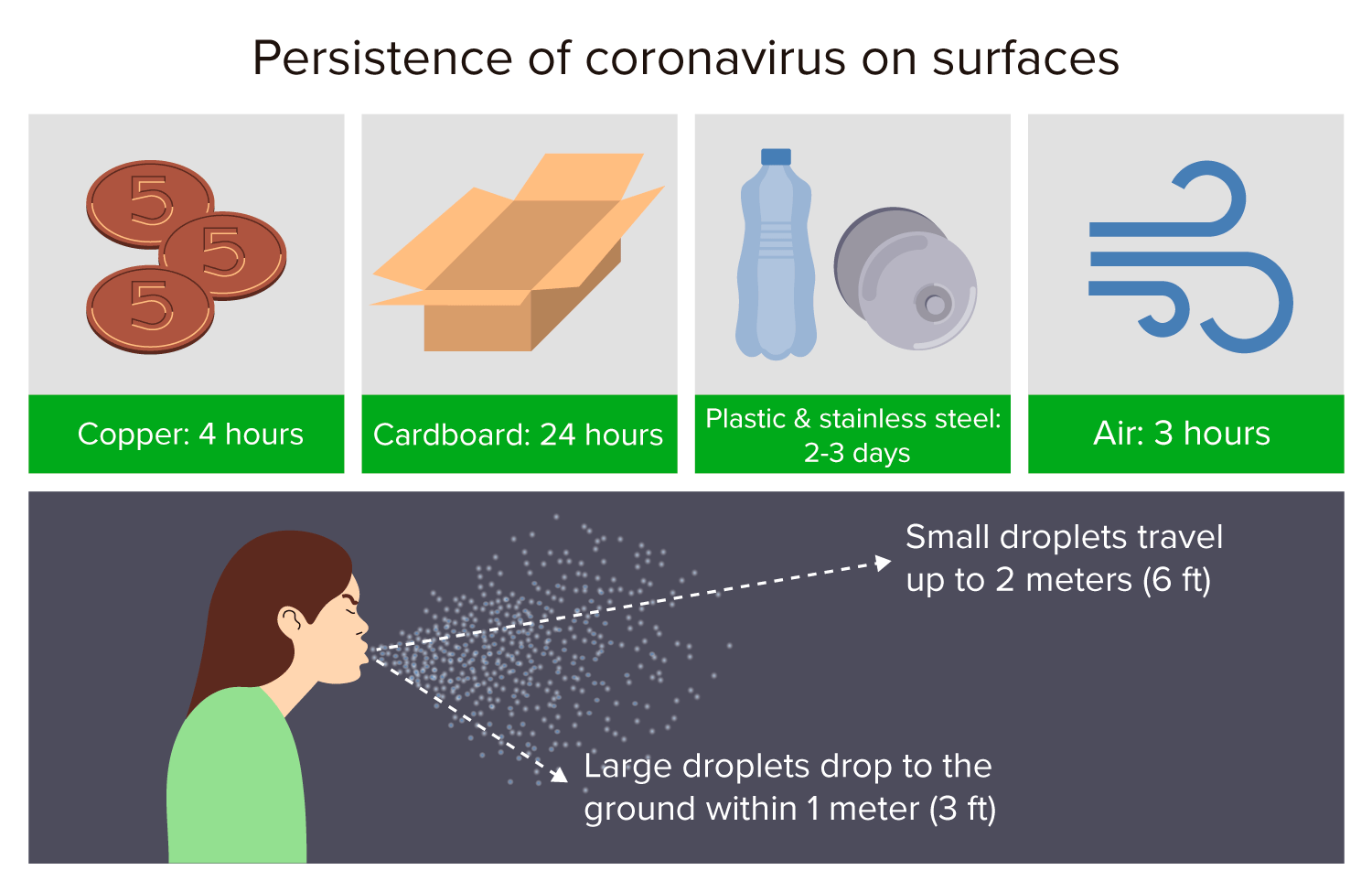
Once in humans, the virus is transmitted mainly via inhalation of aerosol droplets from coughing, sneezing, or talking of symptomatic individuals. In the air, larger droplets tend to drop towards the ground within 1 m (3 ft), while smaller droplets can travel as an aerosol cloud over 2 m (6 ft) and remain viable in the air for up to 3 hours under certain conditions. Other forms of transmission include:
- Direct transmission through hand-to-face contact from infected surfaces
- Fecal-oral transmission is hypothesized (observed in SARS infection, but is still under investigation)
- Vertical transmission (mother-to-child) hasn’t been reported
The period of highest infectivity for symptomatic cases ranges from 2 days before the onset of symptoms up to 3 days after their resolution. (exact limits are still under investigation).
The reproductive number (R0), or the number of secondary infections generated from 1 infected individual, is 2 to 2.5, higher than for influenza (0.9-2.1). COVID-19 is highly contagious due to the following aspects:
- Asymptomatic individuals are also infectious, albeit to a slightly lesser degree, posing a real challenge for contagion prevention.
- Production of high viral loads
- Efficient and prolonged shedding of virions from the upper respiratory tract (URT)
- Median duration of viral RNA shedding from URT: 20 days
- Can remain infectious on surfaces outside a host from a few hours up to a few days.
- Viral life-span depends on the type of surface, temperature, and humidity levels
- There is currently no evidence to suggest that COVID-19 can be acquired from mail and packaged goods.
Epidemiology
The first case of COVID-19 was traced back to Wuhan, China, in late November 2019, with an outbreak developing in December. The virus quickly spread, with widespread ongoing transmission occurring globally. More than 1 million people were infected and over 55,000 died within the first 4 months of global spread. COVID-19 was characterized as a pandemic on March 11, 2020.
Coronavirus COVID-19 Global Cases by Johns Hopkins CSSE. https://www.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6.
Clinical Presentation
- 80% of infections are mild or asymptomatic
- 15% are severe infections (requiring oxygen therapy)
- 5% are critical infections (requiring ventilation)
This proportion of severe and critical to mild cases is higher than in influenza infections.
Asymptomatic cases:
- Can transmit the virus
- Represent >50% of all infections (still under investigation)
- May not develop any noticeable symptoms
- Anosmia, hyposmia, and dysgeusia have been reported in many laboratory-confirmed cases of patients that were otherwise asymptomatic.
- It has not been clearly determined how long asymptomatic individuals remain contagious after initial infection.
Mild cases:
- Dry cough and moderate fever
- Common flu-like symptoms, including fatigue, malaise, runny nose, nasal congestion, and sore throat
- Less frequently: diarrhea, nausea, vomiting, diffuse abdominal pain, productive cough, headache, and muscle or joint pain
- Recovery time: ~2 weeks
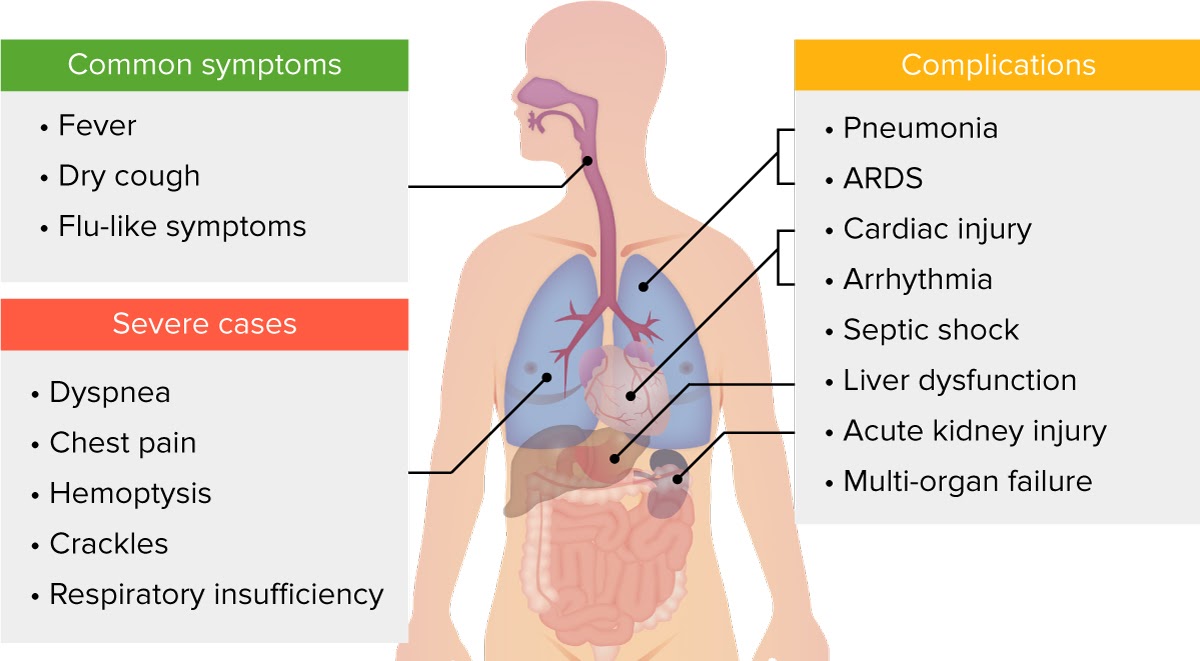
Image: by Lecturio
Severe cases and complications:
- ~1 in 6 people with COVID-19 experience clinical deterioration and/or develop a complication in the 2nd week of illness
- Median time from onset of symptoms to the onset of critical care/ICU transfer: 8-9 days
- Patients develop dyspnea, high fever, chest pain, hemoptysis, respiratory crackles, and progressive respiratory failure
- Recovery time: ~3-6 weeks
Common complications of COVID-19: viral/interstitial pneumonia, acute respiratory distress syndrome (ARDS), sepsis, and septic shock. Other complications: cardiac injury, arrhythmia, liver dysfunction, acute kidney injury, and multi-organ failure.
Risk factors for the severe form and complications of COVID-19:
- Immunosuppression (from long-term steroid use, cancer, AIDS/HIV infection, congenital immunodeficiency, use of immunosuppressants, etc.)
- Age > 65 years
- Chronic diseases (especially hypertension, diabetes mellitus, coronary heart disease, and cerebrovascular disease)
- Pregnancy
The expression of ACE2 is highly increased in patients being treated with ACE inhibitors or angiotensin II type 1 receptor blockers (ARBs). Contrary to initial reports, the American College of Cardiology has pointed out that there is no data to support the claim that ACE inhibitors and ARBs increase the risk of COVID-19 infection, and recommends that patients who already use these medications should continue to do so while further studies are performed.
Refractory cases:
Nearly 50% of COVID-19 patients did not achieve clinical and radiological remission within 10 days of hospitalization. Patients with male sex, older age, anorexia, and no/low fever at the time of admission have a higher risk of presenting a refractory progression.
Related Video Courses:




Diagnostics
Polymerase chain reaction (PCR) is currently the only test being used to confirm cases of COVID-19 infection and should be performed as soon as possible once a person under investigation (PUI) is identified. The specimens used for testing include:
- Nasopharyngeal (NP) and/or oropharyngeal (OP) swab (for mild or asymptomatic suspected cases)
- NP is the first choice. OP swabs are acceptable only if other swabs are not available.
- Can be negative initially. If suspicion of COVID-19 remains, retest every 2-3 days.
- In severe cases, NP and OP swabs may be negative, while specimens from the lower respiratory tract are positive.
- Sputum (for patients with productive cough, inducing is not recommended)
- Bronchial and tracheal secretions or bronchoalveolar lavage (for patients receiving invasive mechanical ventilation)
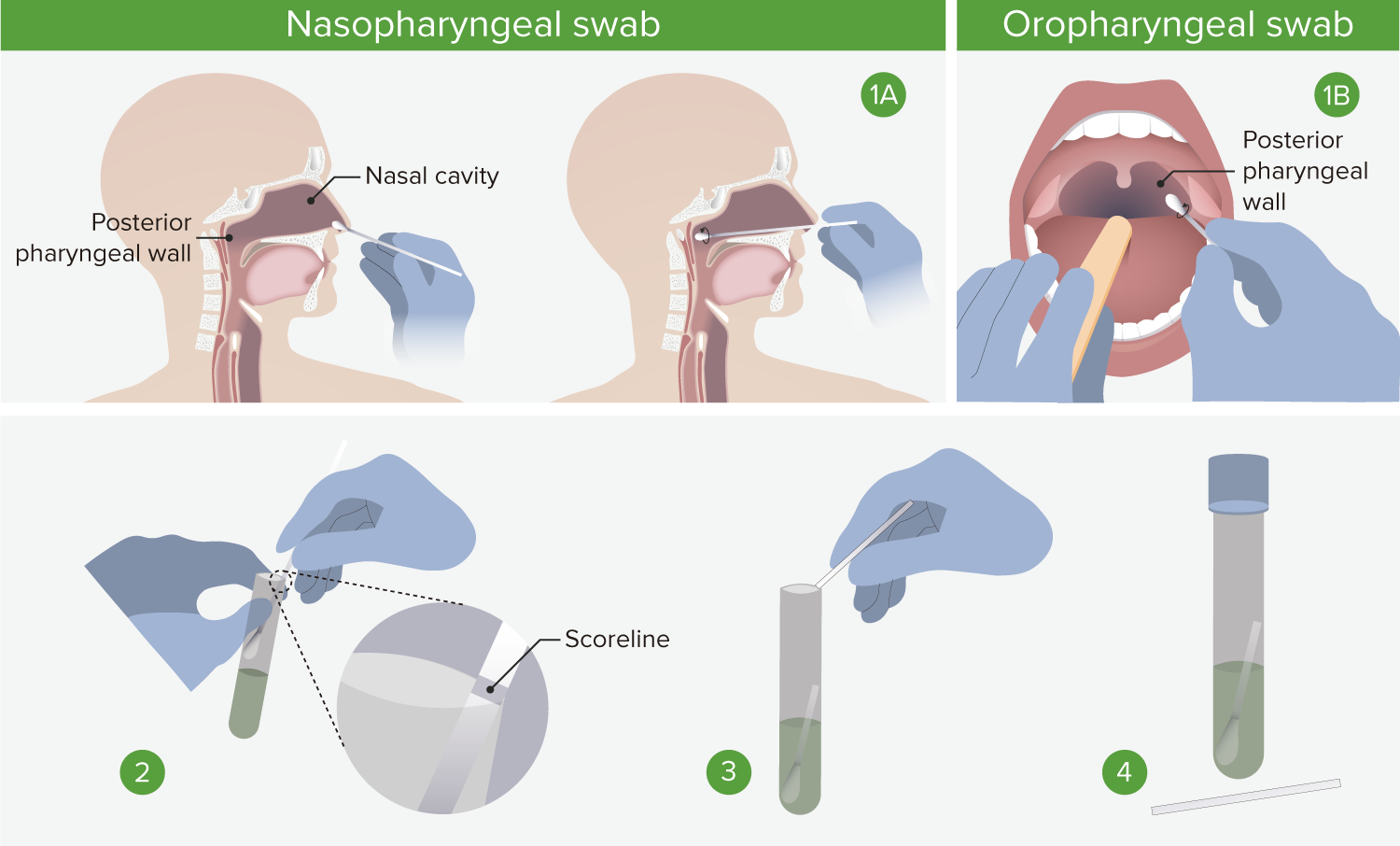
1. Nasopharyngeal swab: Insert swab into a nostril parallel to the palate, and carefully slide it forward until a soft resistance is felt. Swab should reach a depth equal to distance from nostrils to outer opening of the ear. Rotate for several seconds to absorb secretions, and then slowly remove. 1. Oropharyngeal swab: Insert swab into the oral cavity without touching the gums, teeth, and tongue. A tongue depressor may be used. Swab the posterior pharyngeal wall using a rotatory motion. 2. Place swabs immediately into sterile tubes containing 2-3 ml of viral transport media. If both swabs are collected, they should be combined into a single vial. 3. Carefully leverage the swab against the tube rim to break the shaft at the scoreline. 4. Store specimens at 2-8°C for up to 72 hours after collection. If a delay in testing/shipping is expected, store specimens at -70°C or below. Use only synthetic fiber swabs with plastic shafts. Calcium alginate swabs or swabs with wooden shafts may inactivate the virus and inhibit PCR testing.
During an ongoing COVID-19 outbreak, laboratory testing should be prioritized as follows according to the CDC:
- Hospitalized patients with compatible signs and symptoms (especially those presenting with unexplained viral pneumonia or respiratory failure)
- Healthcare professionals with compatible signs and symptoms
- Symptomatic individuals who are at high risk of developing a severe form of the disease or a complication (e.g., patients who are elderly, immunocompromised, or have chronic conditions)
- Critical infrastructure workers with compatible signs and symptoms
- Any individual, including healthcare professionals, who had close contact with a suspect or laboratory-confirmed COVID-19 patient within 2 weeks of their symptom onset, or has a history of travel from affected geographic areas in the last 2 weeks.
- Individuals without symptoms
All persons under investigation (PUI) and confirmed cases should be reported according to regulations set forth by local health authorities and the national surveillance center.
Patients with COVID-19 present with the following laboratory and radiological findings. These are more pronounced and common in severe cases but can be present even in mild infections.
- WBC count: leukopenia, leukocytosis, and lymphopenia (most common)
- Inflammatory markers: ↑ LDH and ferritin
- Liver markers: ↑ AST and ALT
- Chest x-ray and CT: non-specific imaging findings most commonly found in atypical or organizing pneumonia, with a bilateral, peripheral, and/or basal distribution
- Multiple areas of consolidation
- Ground-glass opacities (GGOs)
- Crazy paving appearance (GGOs + inter-/intralobular septal thickening)
- Bronchovascular thickening
In hospitalized COVID-19 patients with severe infections, regular laboratory testing and imaging are necessary for the assessment of disease progression and complications.
- CBC: severe cases present with advanced lymphocytopenia and thrombocytopenia
- ABG: to assess levels of hypoxia and acid-base balance
- ARDS presents initially as hypoxemic respiratory failure with low PaO2 and respiratory alkalosis, later progressing into hypercapnic respiratory failure.
- Inflammatory markers:
- ↑ IL-6 and C-reactive protein in severe cases
- ↑ procalcitonin in bacterial coinfection with pneumonia and/or sepsis
- ↑ lactate in sepsis and septic shock
- Hemostasis tests:
- Prolonged PT and PTT times
- ↑ D-dimer in cardiac injury and septic shock
- Assessment of organ function: abnormal findings may indicate multi-organ failure
- Creatinine, urea, and BUN used to assess renal function
- AST, ALT, GGT, and bilirubin used to assess hepatic function
- Troponin and ECG used to assess cardiac function
- Chest X-ray and CT: severe infections may also present
- Pleural thickening and effusion
- Lymphadenopathy
- Air bronchograms and atelectasis
- Solid white consolidation
Causes of death in COVID-19 patients include progressive hypoxia, multi-organ failure, and hypotensive shock.
Differential Diagnoses
| COVID-19 | Influenza | Common cold | |
|---|---|---|---|
| Incubation period | 2–14 days | 1–4 days | <3 days |
| Onset | Gradual | Sudden | Sudden |
| Fever | Very common | Very common | Rare |
| Dry cough | Very common (mild to severe) | Very common (mild to severe) | Common (usually mild, can be productive) |
| Fatigue | Common | Very Common | Rare or mild |
| Myalgia | Common | Very Common | Mild |
| Sneezing | Sometimes | Rare or mild | Very common |
| Nasal congestion | Rare or mild | Common | Very common |
| Headache | Sometimes | Very common | Rare or mild |
| Sore throat | Sometimes | Sometimes | Very common |
| Diarrhea | Sometimes | Sometimes | Rare |
| Dyspnea | Common | Rare | Never |
Management
No specific treatment for COVID-19 is currently available. As a healthcare professional, one must always implement practices for infection prevention and control (IPC) whenever dealing with a PUI or laboratory-confirmed COVID-19 case.
Patients with mild symptoms and no risk factors do not require hospitalization and are recommended to begin supportive at-home care. In the case of antipyretics, the use of ibuprofen is now considered safe according to the latest WHO advice (March 17, 2020). In the outpatient setting, one must seek professional medical assistance if any of the following emergency warning signs develop:
- Difficulty breathing or shortness of breath
- Persistent pain or pressure in the chest
- Confusion or inability to arouse
- Cyanosis (bluish-tint to lips or face)
The decision to monitor a patient in the inpatient setting should be made on a case-by-case basis. Once hospitalized, supportive care and acute measures should be applied as necessary for complications, such as:
- Oxygen therapy for patients who develop respiratory distress, hypoxemia, or shock
- Empiric antimicrobials in the case of sepsis or secondary pneumonia
- Glucocorticoids have been associated with an increased risk for mortality or severe forms of illness in patients with influenza and MERS-CoV infection. Therefore, the WHO and CDC recommend glucocorticoids not be used in patients with COVID-19 pneumonia unless there are indications related to underlying chronic conditions.
- Advanced oxygen therapy, ventilatory support, and conservative fluid management in the case of acute respiratory distress syndrome
- Fluid bolus and vasopressors in the case of septic shock
For the latest step-by-step management guidelines, see the “WHO interim guidance on clinical management of severe acute respiratory infection when novel coronavirus (nCoV) infection is suspected.”
The mortality rate of COVID-19 varies across different nations and age groups, with a global average of 5.6%; with 1,279,722 cumulative cases and 72,614 deaths according to the WHO Situation Report-78 on April 7, 2020. Patients >80 years of age have a mortality rate of 15%.
The ongoing pandemic makes it difficult to determine an accurate mortality rate at this time. The mortality rate is assumed to be lower due to many undetected cases (lack of widespread testing in many countries and asymptomatic individuals not seeking to be tested).
Investigational therapies
Several clinical trials are currently being performed to further the development and research of antiviral drugs against SARS-CoV 2. However, it’s important to note that there is no available data as of April 6, 2020, to support the recommendation of any of the following investigational therapeutics for patients with confirmed/suspected COVID-19:
- Remdesivir is reported to have in-vitro activity against SARS-CoV and MERS-CoV by incorporating into nascent viral RNA chains and producing pre-mature termination.
- Chloroquine and hydroxychloroquine, widely-used antimalarial drugs, are reported to block viral entry by inhibiting virus/cell fusion.
- The combined use of hydroxychloroquine and azithromycin, a macrolide antibiotic, was reported to reduce the detection of SARS-CoV-2 RNA in upper respiratory tract specimens. Caution is advised when administering these drugs in patients with chronic medical conditions as both are associated with QT prolongation and may lead to life-threatening arrhythmia or sudden death.
- Lopinavir-ritonavir, a combined protease inhibitor usually used for HIV infection, was reported as having in vitro inhibitory activity against SARS-CoV. However, no benefit was observed in hospitalized adult patients with severe Covid-19 in trials conducted in China.
- Tocilizumab is an anti-IL-6 receptor agent used for rheumatoid arthritis. It is currently being investigated in patients with severe COVID-19 presenting with high IL-6 levels.
-
Camostat mesilate (CM): a TMPRSS2 inhibitor, is reported to block viral entry by inhibiting S protein priming.
For more information on international clinical trials, see the WHO website and clinicaltrials.gov
Related Videos:

Prevention
Individuals who live within an area undergoing an outbreak are advised to prevent the spread of COVID-19 infection. General recommendations include:
- Home isolation and/or avoiding public/crowded areas whenever possible to minimize the chance for exposure
- Covering coughs and sneezes with a tissue or the inner elbow
- Washing hands regularly for at least 20 seconds with soap and water or with an alcohol-based hand sanitizer that contains at least 60% alcohol
- Maintain 1–2 m (~3–6 ft) distance from other people, “social distancing”
- Regular cleaning of all ‘high-touch’ surfaces within the home
- Wearing a facemask if one is a healthcare professional, begins to present with symptoms, or when caring for a sick individual. The use of facemasks is not recommended for the general population.
Isolation and quarantine can be discontinued only after the following criteria has been met:
- For hospitalized patients: negative results of PCR testing from at least 2 consecutive sets of paired nasopharyngeal and throat swab specimens collected ≥ 24 hours apart (total of 4 specimens: 2 nasopharyngeal and 2 throat)
- For at-home patients: negative results of PCR testing from at least 2 consecutive nasopharyngeal swab specimens collected ≥ 24 hours apart OR
- At least 3 days have passed since the resolution of fever without the use of antipyretics and improvement in respiratory symptoms AND
- At least 7 days have passed since the onset of symptoms
For more detailed guidelines on how to prevent infection, see the Interim Infection Prevention and Control Recommendations for Patients with Suspected or Confirmed Coronavirus Disease 2019 (COVID-19) in Healthcare Settings (CDC).
Vaccine:
There is no FDA-approved vaccine yet available to prevent COVID-19. A Phase 1 clinical trial evaluating an investigational vaccine began on March 16, 2020, in the Kaiser Permanente Washington Health Research Institute (KPWHRI) in Seattle, WA, USA. The vaccine is called mRNA-1273, and is designed to encode for a prefusion-stabilized form of the S protein. The trial will enroll 45 healthy adult volunteers aged 18 to 55 years over approximately 6 weeks.
References:
www.who.int/health-topics/coronavirus
www.cdc.gov/coronavirus/2019-nCoV/hcp/index.html
coronavirus.jhu.edu/map.html
www.thelancet.com/journals/lanres/article/PIIS2213-2600(20)30116-8/fulltext
www.nature.com/articles/nm1267
www.biorxiv.org/content/10.1101/2020.03.14.988345v1
www.ncbi.nlm.nih.gov/pmc/articles/PMC6893680/
www.ncbi.nlm.nih.gov/pmc/articles/PMC4369385/
www.journalofhospitalinfection.com/article/S0195-6701(20)30046-3/fulltext
mmrjournal.biomedcentral.com/articles/10.1186/s40779-020-00240-0
www.thelancet.com/journals/laninf/article/PIIS1473-3099(20)30232-2/fulltext
www.ncbi.nlm.nih.gov/pubmed?term=32109013
academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa270/5805508
www.cell.com/cell/fulltext/S0092-8674(20)30229-4?rss=yes#secsectitle0065

 留言列表
留言列表

